A few months after the Civil War began, on July 4, 1861, a group of patriotic young volunteers stood in the shadow of the Capitol, waiting to be sworn into the Union Army on a 90-day enlistment. Among them was William W. Keen. Less than three weeks later, and with only nine months of medical training, Keen stood clueless, in his blue uniform with the green sash of a medical officer, near the battlefield at Bull Run in Virginia.
“It was an exceedingly hot day, and we marched and halted in the thick dust under a broiling sun until about noon. . . . During the entire engagement, I never received a single order.” Inside a church he and fellow soldiers placed two boards on boxes in front of a pulpit for an operating table. Hearing that the Confederates were about to overrun the makeshift hospital, Keen’s patient, a soldier with a fractured humerus from a Minié ball (a powerful new rifled bullet), jumped up and ran for the woods, his bandage unraveling from his arm as he went. Keen later wrote, “My experience in this battle is a good illustration of the utter disorganization, or rather want of organization, of our entire army at the beginning of the war.”

Had Keen received an adequate briefing before battle, he would still have been left frustrated with a medical infrastructure unchanged in its essentials since the Mexican War of the 1840s. His experience typified the Federal government’s lack of preparedness in wartime. In fact, the lack of infrastructure, particularly ambulances, meant that many Bull Run casualties waited for days on the battlefield before soldiers or civilians removed them to hospitals.
At Bull Run, Keen received a crash course in misery. Battlefield hospitals were triage centers: stacks of amputated limbs marked the surgeons’ tents. Soldiers with severe abdominal or chest injuries were left to die: no surgical intervention was possible without the sure consequence of infection. The soldier’s life may have been punctuated with combat terror, but disease and illness afflicted far more troops than did battlefield wounds. Germ theory and antisepsis entered medicine only after the war. Counting deaths from wounds or disease, the war claimed between 600,000 and 700,000 lives, more than the number of soldiers killed in all other American wars combined. Beyond battlefield wounds, soldiers suffered malnutrition (including scurvy), dysentery, typhus, typhoid, respiratory illnesses, rheumatism, and outbreaks of malaria, yellow fever, and even smallpox (despite the prevalence of vaccination).
By the end of the war a radical reorganization of the medical field had occurred. The Medical Department could boast of an ambulance system, a sequence of care facilities from battlefield surgery to general hospitals, evacuation of the sick and wounded by train, and a nascent nursing profession. A new system—of government-funded pharmaceutical research and manufacturing—had taken hold. The demand for new chemical and botanical sources for medicines and for the production of reliable vaccines accelerated laboratory-based research and guided postwar pharmacology—including the growth of major manufacturing firms John Wyeth and Eli Lilly. In addition, Civil War pharmacology produced competing therapies and bitter disagreements that brought the Union Army surgeon general to court-martial and established the position of one of the most versatile and effective medicines of the late 19th century: quinine.
Hospital Systems
On July 21, however, Keen was unable to benefit from these future developments. During the fall of 1861 he went to Philadelphia to complete his formal studies, which at that time required a year of anatomy classes, which was then repeated and followed by several years of apprenticeship with an established physician. Keen returned to the army to find the medical service invigorated. The military had created a cadet corps, a comprehensive examination procedure, and a training school, and decided rank and assignments based on merit. Although Keen had a good knowledge of materia medica—pharmacy—the army’s organization of medicine might have impressed him with its diversity and complexity. Physicians generally relied on the Supply Table—the army’s standard table of drugs, their effects, and their preparation for use. During the war the army created a system that began with acquiring raw materials (eventually creating its own laboratories), included quality control, continued with the preparation and distribution of medicines to armies in the field or to hospitals, and went on to a method of prescribing and dispensing to ill soldiers.
Initially, both the Union and Confederate armies immediately distributed any medicines purchased. Later, the Union Army purchased raw materials, such as cinchona bark for quinine, for processing at its own or contract laboratories. The South, with no drug-manufacturing centers, was forced to smuggle medicines, capture them, or invent alternatives. When Keen required medicine for his patients, medical purveyors—usually a military officer or physician—bought drugs on the market or obtained them from one of many depots, and then shipped them; medical storekeepers took receipt and stored medicines until needed; surgeons wrote prescriptions; and in the Union Army hospital stewards filled them. With a rank equivalent to a sergeant the hospital steward was an apothecary who supervised lesser hospital staff and occasionally performed minor surgery. As the war progressed, purveyors for the Union Army learned which wholesalers or companies delivered trustworthy and reliable products. The most influential laboratories serving the Union Army included Charles Pfizer and Company, Edward R. Squibb, Schief¬felin and Company, Powers and Weightman (many years later to become Merck), Rosengarten and Sons, and John Wyeth—many of which still dominate the industry today.
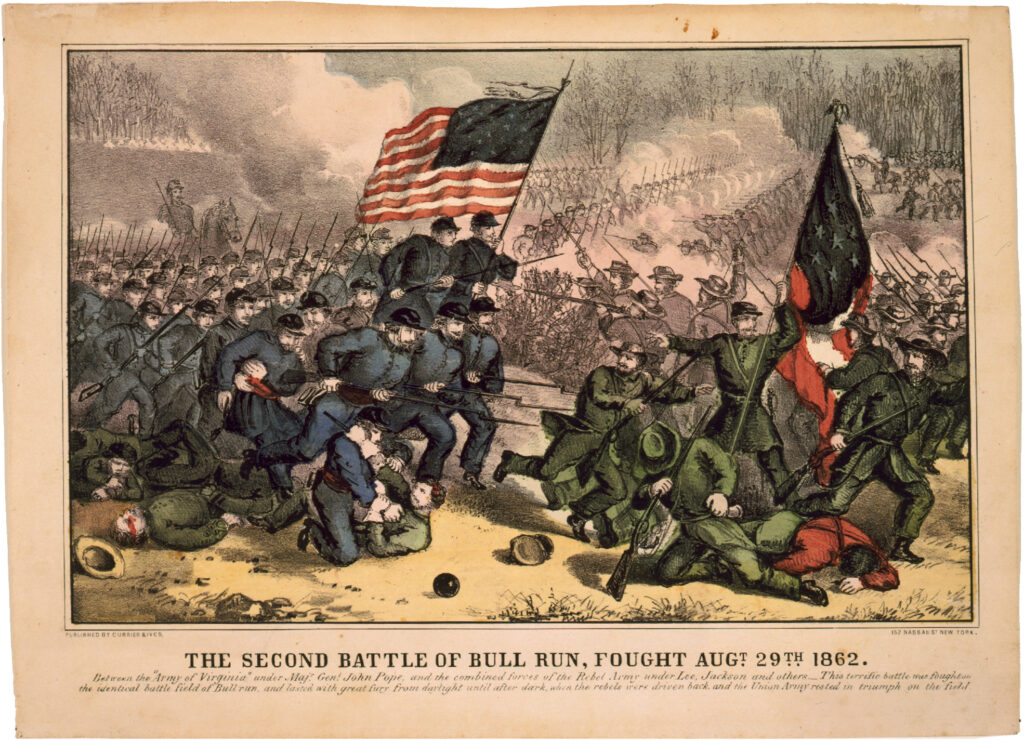
These developments formed the background of a desperate war. A year after Bull Run, Keen found himself back for the Second Battle of Bull Run. He set up a field hospital at nearby Centreville “and soon afterward began to distribute the instruments, blankets, medicines, stimulants, etc., I had brought. . .. Before I left Washington I had been directed to be rather sparing in distributing these, and I obeyed orders.” He regretted his parsimony when a regiment of Virginia Confederate Cavalry overran the field hospital. Keen was forced to hand over the key to the storehouse of “medicines, stimulants, operating cases, and . . . more valuable things that I had brought along—how their eyes widened and their faces were wreathed in smiles as the doctor, after a rapid survey of the boxes on the walls, turned to the colonel and said, with an expletive: ‘There is more good whiskey in this little smoke-house than there is in the whole city of Richmond!’”
Stranded with about 100 wounded men without supplies, Keen surveyed the misery. Some pitying Confederates even donated canned soup. He received important assistance from two Northern quasi-governmental relief organizations, the U.S. Christian and U.S. Sanitary Commissions, both of which showed up with food. While others prepared soup, Keen “took a bottle of morphine and [his] pocket penknife and did not worry over any superfluous exactitude in doling out the blessed relief which morphine brings to men in pain. All of this was done in total darkness, with two or three slim lanterns, in a drizzling rain, and in six inches of Virginia mud.” Keen faced rampant infections owing to severe internal injuries. “Wounds of the abdomen involving the viscera were almost uniformly fatal. . . . Opium was practically our only remedy [for abdominal surgery] and death the usual result.”
Pharmaceutical Development
In 1862 Jonathan Letterman, medical director of the Army of the Potomac, ordered Keen to commandeer two Washington, D.C., churches and convert them into hospitals in five days. Keen complied, but the army way of doing things remained obscure. “I was not lacking in ordinary intelligence and was willing to work, but I was utterly without training. . . . As to drugs I did not know whether to order six ounces or a gallon of laudanum, an ounce or two or a pound or two of opium.”
The pharmacopoeia at Keen’s disposal, which centered on the Supply Table, presented a sophisticated constellation of substances. Nineteenth-century understanding of the origins of disease is both familiar and strange; the restoration of balance within bodily systems, a relic of humoral theory (in which black bile, yellow bile, blood, and phlegm made up the humors), still informed much of medicine. The category of “fevers” represented a type of disease rather than a symptom. Some diseases, such as typhoid and typhus, were not easy to distinguish, and as a result received identical treatments.
In the hospital Keen wrote prescriptions in Latin, the universal custom, and gave them to the steward to compound. To a 21st-century pharmacist, some of the substances popular then, like Dover’s Powder and calomel—the former containing opium, the latter, mercury—have no recommended therapeutic purpose. Some, like antimony- and lead-based drugs, are downright dangerous, while others remain in use—such as iodine and quinine. With no laboratory methods available to establish drug usefulness through testing, no systematic antisepsis, and no germ theory, Keen worked within a system of medical knowledge based on observation of symptoms rather than causes.
Many of the soldiers Keen saw at his Washington hospitals arrived not only ill or wounded but debilitated by poor nutrition and the harsh physical demands of campaigning. Keen was harrowed by the sight of sick soldiers. After the Second Battle of Bull Run he wrote: “I passed such a night as I had never before experienced in my life. Long trains of ambulances arrived, carrying our wounded from the field of battle. . . . Fifty poor, thirsty fellows were crying for water; fifty more were crying with the pain from a jolting ride [to Washington] of nine miles over a corduroy road. Most of them had had nothing to eat for one, two, or three days, save what they had obtained from the haversacks of poor fellows who were dead in their neighborhood. Some had such horrible wounds that they could absolutely go no farther, and must be got out on stretchers and taken into the hospital.”
Given the major role illness played in war, military strategy had to weigh the health of entire regiments; every soldier suffered diarrhea at least once, and many experienced dysentery. Patients at Keen’s hospital were fed a healthy, vegetable-rich diet. Calomel and opium were also favored treatments. He wrote later, “What we did not have in those days was almost more noticeable than what we did have. Among our blessings, however, were ether and chloroform. . . . We had, however, no antiseptics, for antisepsis was as yet even undreamed of.” He classified fevers as common, remittent, or intermittent, some of which accompanied dysentery or may have been symptomatic of typhus or typhoid, both of which flourished in the unhygienic camps. Keen prescribed quinine or cinchona for the fevers associated with both, just as he might have for malaria. Where Keen saw the most life-threatening respiratory disease, pneumonia (then recognized as an inflammation of the lungs), he may have prescribed tartar emetic or antimony, a therapy that became the focus of a controversy within the Union Army Medical Department.
Quinine proved the true medicinal miracle of the war. Malarial fevers were omnipresent during Southern campaigns, and the Union Army’s mandated prophylactic use of quinine prevented much illness, a benefit widely lauded by military commanders. Rosengarten and Sons, a major drug supplier to the Union Army in Philadelphia, excelled at producing quinine. The company employed French chemists versed in the techniques of isolating the alkaloid quinine, a process worked out 40 years before the war.
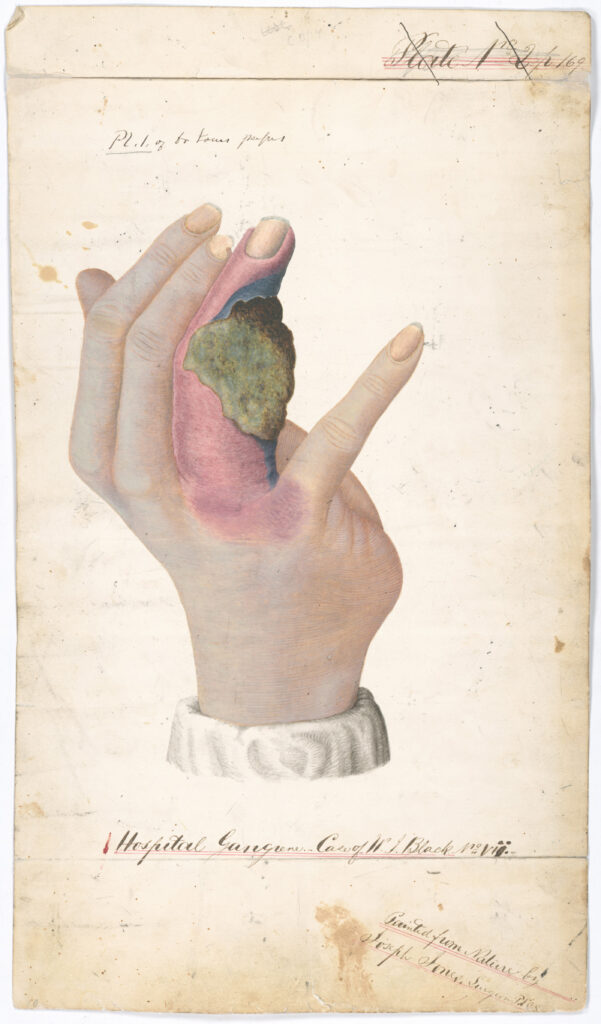
Hospitals were not always safe for patients. Keen worried about outbreaks of “hospital gangrene” owing to staphylococcus or other causes not known at the time. Gangrenous patients were immediately removed and isolated, and Keen may have ordered an effective treatment recognized during the latter part of the war: bromine. Mortality from these infections approached 97%. Worse than these diseases—from a military commander’s viewpoint—were epidemics. Yellow fever and smallpox epidemics afflicted both civilian and military populations in the North and South. Both armies required military recruits to be vaccinated for smallpox, but vaccine supplies were irregular and of uncertain quality. In the absence of vaccines some soldiers practiced the 18th-century technique of variolation, that of removing lymph from a smallpox-infected person and introducing it subcutaneously (with a knife) to others to engender a hopefully mild infection.
The battlefield presented even more challenges. At Gettysburg, with almost 30,000 soldiers awaiting treatment, Keen probed a soldier’s gunshot wound near the upper shoulder and neck, trying to stop the bleeding. “The bullet had not emerged; its direction was unknown; the hemorrhage was profuse. . . . I etherized the man and proceeded to search for the wounded vessel.” Contrary to popular opinion, more than 95% of major Civil War surgeries were performed under ether or chloroform. Ether’s flammability, however, was yet another danger. “My only light was a square block of wood with five auger holes,” Keen continued, “in each one of which was placed a candle. . . . As the wound was so near the mouth, of course the light had to be near the ether cone [the mask placed over the patient’s face to receive the anesthesia]. . . . Suddenly the ether took fire and the etherizer flung away both cone and bottle. Luckily the bottle did not break or we might have had an ugly fire in a hospital constructed wholly of wood.”
Medical Victories
The chief medical achievements during the war were organizational. Apart from the banning of mercury, wartime medicines underwent little change until germ theory became understood. At first physicians applied medicines based on their own observations of the results, which created different philosophies of medication. The huge demand for drugs during the war allowed physicians to investigate and study the effectiveness of their pharmacopoeia more systematically and created the infrastructure for large-scale drug manufacturing and testing. As the federal government operated processing laboratories, government support and testing gradually became more important. Quinine and its various forms were abundantly tested, and their value was confirmed.
The distance in time between the beginning of World War II and today is equivalent to the time between the end of the Civil War and the beginning of World War II—not so long, but distant in medical ideology and practice. Keen’s wartime practice heeded the holistic perspective demanded by medical director Jonathan Letterman, who pointed out “that the duties of Medical officers are not confined to prescribing drugs, but that it is also their duty . . . to preserve the health of those who are well. . . . The prevention of disease is the highest object of medical science.”
Keen himself, the only physician to serve in uniform in both the Civil War and World War I, participated in the transformation of American medicine and therapeutics into the 20th century. He eagerly embraced antisepsis and germ theory, kept current with such new technologies as X-rays, and abandoned counterproductive medicines. Recollecting the War of the Rebellion, as he called it, “Only too sharply do we remember the dreadful things that we did do and the good things that we did not dare to do.”


